
Is Lifting Heavy Weights Safe for Women Over 40? What the Research Actually Says
- Nikolay Atanasov
- Apr 28
- 11 min read

Updated: May 19

QUICK READ: THE DATA
The direct answer: Yes, appropriately progressed resistance training — including challenging loads — is safe for women over 40, including those with low bone density. The research is unambiguous on this point.
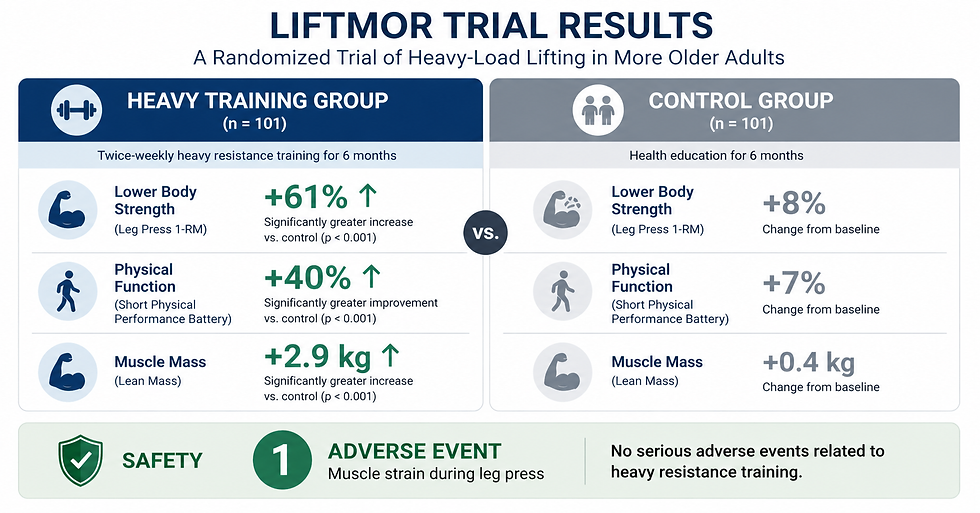
The landmark study: The LIFTMOR trial tested heavy resistance training (5 sets of 5 reps at >85% of 1RM) in postmenopausal women with osteopenia and osteoporosis for 8 months. Result: only one adverse event (a minor lower back spasm that caused 2 missed sessions out of 70). Compliance was 92%.
The results: The heavy-lifting group saw lumbar spine bone mineral density increase by 2.9% while the control group lost 1.2%. Femoral neck BMD, functional performance, and even height all improved significantly.
The institutional consensus: The National Strength and Conditioning Association's 2019 position statement (663 citations) concludes that resistance training is beneficial and safe for older adults with proper instruction and individualized progression.
The practical point: "Heavy" is relative to your starting strength. A challenging bodyweight squat is heavy for a beginner. The principle is progressive overload — making the exercise hard enough that your muscles are genuinely challenged — not a specific weight on a barbell.
The fear of lifting heavy after 40 is one of the most persistent and damaging myths in women's fitness. It keeps women doing light-weight, high-rep circuits and long cardio sessions — exactly the training that does not prevent the muscle loss, bone loss, and strength decline that accelerate after menopause.
The research tells a completely different story: appropriately progressed, challenging resistance training is not only safe for postmenopausal women — it's one of the most effective interventions available for bone density, muscle strength, and physical function. The evidence base includes randomised controlled trials in women who already have weak bones — the exact population you'd expect to be most at risk. (Source: Watson et al., LIFTMOR trial, J Bone Miner Res, 2018)
This article walks through what the research actually found, what makes resistance training safe or unsafe, where the fear comes from, and how to apply the evidence — including at home, without equipment. For the specific exercises, see the strength exercises that protect against muscle loss.
What Did the LIFTMOR Trial Actually Find?
The LIFTMOR trial (Lifting Intervention For Training Muscle and Osteoporosis Rehabilitation) is the most important single study on this topic, because it deliberately tested what conventional wisdom said was too dangerous.
The study recruited postmenopausal women with low to very low bone mass (T-score below -1.0 — meaning osteopenia or osteoporosis) and randomised them to either 8 months of twice-weekly, 30-minute, supervised high-intensity resistance training (HiRIT) or a home-based low-intensity exercise programme. The HiRIT protocol was genuinely heavy: 5 sets of 5 repetitions at greater than 85% of one-repetition maximum. (Source: Watson et al., 2018)
The results:
Outcome | Heavy Training Group | Control Group | Significance |
Lumbar spine BMD | +2.9% | -1.2% | p < 0.001 |
Femoral neck BMD | +0.3% | -1.9% | p = 0.004 |
Femoral neck cortical thickness | +13.6% | +6.3% | p = 0.014 |
Height | +0.2 cm | -0.2 cm | p = 0.004 |
All functional performance measures | Significant improvement | No significant change | p < 0.001 |
Compliance | 92% | 85% | — |
Adverse events | 1 (minor back spasm, 2 sessions missed) | 0 | — |
The authors' own conclusion: "Contrary to current opinion, HiRIT was efficacious and induced no adverse events under highly supervised conditions for our sample of otherwise healthy postmenopausal women with low to very low bone mass." (Source: Watson et al., 2018)
Read that again: women with osteoporosis lifting at >85% of their max, twice a week for 8 months, with one minor back spasm across the entire study. The lumbar spine — the site most at risk for compression fractures — gained nearly 3% in density while the control group lost more than 1%.
Why Conventional Guidelines Were Too Conservative
Prior to LIFTMOR, most exercise guidelines for women with osteoporosis recommended moderate-intensity exercises only, owing to a perceived risk of fracture from high-intensity loading. The researchers explicitly noted that this conservative approach produced disappointing bone outcomes. The LIFTMOR protocol — deliberately designed to challenge that conventional wisdom — showed that bone tissue responds preferentially to high-magnitude forces, not moderate ones. Avoiding heavy loading to "protect" fragile bones may actually deprive them of the stimulus they need to get stronger.
What Do the Major Fitness and Medical Organisations Say?
The LIFTMOR trial isn't an outlier. The institutional consensus aligns with it.
The National Strength and Conditioning Association (NSCA) published its first-ever Position Statement on Resistance Training for Older Adults in 2019, backed by 663 research citations. The statement concluded that resistance training is beneficial and safe for healthy older adults when performed with proper instruction. (Source: Fragala et al., J Strength Cond Res, 2019)
The NSCA's specific recommendations for older adults: incorporate resistance training 2–3 times per week; perform 2–3 sets of 8–10 exercises targeting major muscle groups; work at 70–85% of 1RM for strength development; follow an individualised, periodised progression. The statement explicitly noted that injuries in older adults are mainly related to heavy and repetitive workload combined with incorrect technique — not to heavy resistance per se.
A separate systematic review of resistance training for postmenopausal women confirmed this: across 12 randomised clinical trials involving 452 participants, no serious adverse events were reported. Resistance training produced significant improvements in functional capacity, bone mineral density, upper- and lower-body strength, and reduced hot flash frequency and fat mass. (Source: González-Gálvez et al., Menopause, 2023)
A further systematic review of high-intensity and high-impact exercises in postmenopausal women concluded that these protocols are effective for improving or maintaining bone density in the lumbar spine and femur, and that they were found to be safe in older women with careful supervision. (Source: Cureus, 2023)
What Actually Makes Resistance Training Unsafe?
The evidence is clear that challenging resistance training is safe. But that doesn't mean all resistance training is automatically safe. The NSCA position statement identified the actual risk factors for injury, and none of them are "being over 40" or "being a woman":
1. Incorrect technique under load. This is the primary risk factor. Performing a deadlift with a rounded lower back, or pressing overhead with insufficient shoulder mobility, creates injury risk regardless of age. Technique matters more as load increases.
2. Too much too soon. Jumping from no training to heavy loads without a gradual progression violates the principle of progressive overload. The body needs time to adapt — tendons and connective tissue adapt more slowly than muscles. (Source: Fragala et al., NSCA, 2019)
3. Ignoring pain signals. Working through sharp or persistent pain — particularly in shoulders, knees, or lower back — is a risk factor at any age. After 40, connective tissue is less resilient due to hormonal changes (declining estrogen affects collagen integrity), which makes joint feedback even more important to respect.
4. No periodisation. Doing the same heavy routine without variation in volume and intensity leads to overuse injuries. The NSCA recommends periodised progression — planned variation in sets, reps, intensity, and exercise selection over weeks and months.
5. Underlying medical conditions not accounted for. Uncontrolled hypertension, recent cardiac events, unstable spinal conditions, or active joint inflammation require medical clearance and modified programming — not avoidance of exercise entirely.
"The biggest safety risk for women over 40 isn't training too hard — it's not training at all. Muscle loss, bone loss, and strength decline are not neutral outcomes. They lead to fractures, falls, disability, and loss of independence. The research is overwhelming: appropriately progressed strength training, including genuinely challenging loads, is safer than the consequences of not training. That's the risk calculation most women aren't being given. We built TransformFitAI around progressive bodyweight training specifically because it solves the technique and progression problems that make heavy training risky — while still delivering the intensity the research shows is necessary."
— Nikolay Atanasov, Founder of TransformFitAI
Does "Heavy" Have to Mean Barbells?
No — and this is the practical point that matters most. "Heavy" in the research context means an intensity where the muscles are genuinely challenged in the last few repetitions of a set. For a woman who has never done resistance training, a bodyweight squat is heavy. For a woman who has been training for years, a barbell squat might be required to reach the same relative challenge.
The underlying mechanism is Type II (fast-twitch) muscle fibre recruitment. These fibres only activate when the load is challenging enough — typically in the last 2–3 reps of a set performed close to muscular effort. The equipment is irrelevant; the intensity is what matters. (Source: Verdijk et al., 2013)
Bodyweight progressions — wall push-ups to incline push-ups to full push-ups, chair squats to tempo squats to single-leg variations — follow the same progressive overload principle as barbell training. Each harder variation increases the intensity relative to your current capacity, which is the definition of progressive overload.
This is the key insight that makes strength training accessible: you don't need a gym to train "heavy." You need exercises that are genuinely challenging for your current level of strength, and a system that makes them harder as you get stronger.
How TransformFitAI Makes Challenging Training Safe and Accessible
The safety risks the NSCA identified — poor technique, no progression, ignoring pain, no periodisation — are all programme design problems. TransformFitAI was built to solve them.
Progressive bodyweight training eliminates the technique barrier. Bodyweight exercises are self-limiting — your body is the load, and the movement patterns are natural. There's no barbell to misposition, no weight plate to drop. The risk profile of a push-up progression is fundamentally different from a heavy barbell bench press, while the muscle stimulus — when performed at the right difficulty level — is equivalent for a beginner or intermediate trainee.
The AI controls the progression. Every 14 days, you upload new body scans and the AI advances your programme based on what you've demonstrated you can do. This prevents the "too much too soon" problem by building difficulty gradually and systematically — exactly the periodised approach the NSCA recommends.
Joint-friendly exercise selection respects pain signals. If you report knee, back, or shoulder sensitivity, the AI excludes movements that would aggravate them and substitutes safer variations targeting the same muscle groups. This keeps you training consistently without the injury interruptions that derail most women's progress after 40.
How to Train Safely and Effectively After 40
Start where you are. If you haven't strength-trained before, bodyweight exercises at the right difficulty level are challenging enough to produce adaptation. You don't need a gym.
Progress gradually. Add difficulty every 1–2 weeks: more reps, slower tempo, or a harder variation. Never jump intensity dramatically.
Make the last 2–3 reps genuinely hard. If you can easily complete 15+ reps, the exercise is too easy. Progress to a harder variation. Insufficient challenge means insufficient adaptation.
Respect joint pain — but don't avoid exercise. Sharp or persistent pain in a joint means modifying the movement, not stopping training entirely. Substitute a safer variation for the same muscle group.
Train 3 times per week with at least one rest day between sessions. This matches both the NSCA recommendations and the clinical protocol for postmenopausal women.
Pair training with 20–25g protein per meal. This supports the muscle-building response and partially offsets the blunted anabolic response after menopause.
Get medical clearance if you have: uncontrolled high blood pressure, recent cardiac event, history of stroke, known fracture risk, significant joint pain that affects daily activities, or any condition your doctor has previously flagged.
Ready to train with real Intensity - safely
?
TransformFitAI builds a personalized bodyweight strength programme designed to target the Type II muscle fibres most vulnerable to age-related decline. Progressive overload, joint-safe by design, adapted every 14 days. No gym. No equipment. Try it free for your first day, then $1.99 for your first month.
$1.99 / first month
First training day completely free · 30-day money-back guarantee · Cancel anytime
Frequently Asked Questions About Cardio vs Resistance Training After 40
Is resistance training safe for women with osteoporosis?
Yes, under appropriate supervision and progression. The LIFTMOR trial specifically tested heavy resistance training (5 sets of 5 reps at more than 85% of 1-repetition maximum) in postmenopausal women with osteopenia and osteoporosis over 8 months. The study reported only one adverse event — a minor lower back spasm — with 92% compliance. Lumbar spine bone mineral density increased by 2.9% in the training group while declining 1.2% in controls. The researchers concluded that heavy resistance training was both safe and effective for this population.
Will heavy lifting cause injuries in women over 40?
Injuries in older adults are primarily related to incorrect technique combined with heavy loads, excessive volume without periodisation, and ignoring pain signals — not to heavy resistance training per se. Multiple systematic reviews of resistance training in postmenopausal women have reported no serious adverse events. The NSCA Position Statement on Resistance Training for Older Adults (2019) explicitly states that resistance training is safe with proper instruction and individualised progression.
Is it too late to start strength training at 50 or 60?
No. Research consistently shows significant improvements in strength, muscle mass, bone density, and functional performance in postmenopausal women who begin resistance training, including those who have never trained before. The NSCA Position Statement recommends that beginners start with lighter loads (50–70% of 1RM) and progress gradually to higher intensities. Even once-weekly training produces measurable strength gains in older adults.
Should I see a doctor before starting strength training after 40?
Talk to your physician before starting if you have uncontrolled high blood pressure, a recent cardiac event, a history of stroke, significant joint pain that affects daily activities, a known fracture risk, or any condition your doctor has previously told you limits your exercise. For otherwise healthy women over 40 with no contraindicated conditions, resistance training can be started immediately with appropriate progression. Medical clearance is a precaution for specific conditions, not a requirement for exercise itself.
What does "progressive overload" mean in practical terms?
Progressive overload means gradually increasing the challenge placed on your muscles over time. In practical terms for bodyweight training: start with an easier variation (wall push-ups, chair-supported squats), then progress to a harder one when you can comfortably do 12–15 reps. The harder variation might be a steeper angle (incline push-ups), a slower tempo (3 seconds down, 1 second up), a single-leg version, or simply more reps of the same movement. The key is that each week, the training is slightly harder than the week before.
Does bodyweight training work as well as weight training for reversing strength loss?
Yes, when progressive overload is properly applied. The stimulus that drives Type II fibre adaptation is intensity in the last few reps of a set — not the type of equipment used. Bodyweight progressions (wall push-ups to full push-ups, chair squats to single-leg variations) follow the same progressive overload principle as barbell training. A consistent bodyweight programme performed 3 times per week with ongoing progression produces meaningful strength gains at any age.
Continue Exploring:
Scientific References
Watson SL, Weeks BK, Weis LJ, Harding AT, Horan SA, Beck BR. High-Intensity Resistance and Impact Training Improves Bone Mineral Density and Physical Function in Postmenopausal Women With Osteopenia and Osteoporosis: The LIFTMOR Randomized Controlled Trial. J Bone Miner Res, 2018. PubMed 28975661
Fragala MS, Cadore EL, Dorgo S, Izquierdo M, Kraemer WJ, Peterson MD, Ryan ED. Resistance Training for Older Adults: Position Statement From the National Strength and Conditioning Association. J Strength Cond Res, 2019. PubMed 31343601
González-Gálvez N, Moreno-Torres JM, Vaquero-Cristóbal R. Resistance training for postmenopausal women: systematic review and meta-analysis. Menopause, 2023. PubMed 36283059
Singla S, et al. The Role of High-intensity and High-impact Exercises in Improving Bone Health in Postmenopausal Women: A Systematic Review. Cureus, 2023. PMC9990535
Roberts S, Collins P, Rattray B. Resistance exercise as a treatment for sarcopenia: prescription and delivery. Age and Ageing, 2022. Age and Ageing
Buckinx F, Aubertin-Leheudre M. Sarcopenia in Menopausal Women: Current Perspectives. Int J Womens Health, 2022. PMC9235827
Verdijk LB, et al. The decline in skeletal muscle mass with aging is mainly attributed to a reduction in type II muscle fiber size. 2013. PubMed 23425621
Mitchell WK, et al. Sarcopenia, Dynapenia, and the Impact of Advancing Age on Human Skeletal Muscle Size and Strength. Frontiers in Physiology, 2012. PMC3429036
Medical Disclaimer: TransformFitAI is a general wellness tool and not a substitute for medical advice. The information in this article is for educational purposes. Always consult with your physician before changing your exercise programme, especially if you have cardiovascular concerns, joint conditions, or existing health conditions. Individual results may vary.


Comments